Learn about colorectal cancer surgery – removing tumors from the colon or rectum. We use laparoscopic and robotic methods for smaller cuts, less pain, and faster recovery.
Colorectal cancer surgery removes cancer from the large intestine (colon) or the rectum (the last part of the large intestine). The main surgeries are colectomy (removing part of colon), low anterior resection, and abdominoperineal resection. We perform these using laparoscopic (keyhole) or robotic methods whenever possible.
Colorectal cancer is one of the most common cancers. Early signs include blood in the stool, change in bowel habits (diarrhea or constipation lasting weeks), belly pain, weight loss, and feeling that your bowel does not empty completely. If caught early, surgery offers an excellent chance for cure.
The type of surgery depends on where the tumor is located. For cancer in the right colon, a right hemicolectomy is done. For the left side, a left hemicolectomy or sigmoid colectomy is performed. For rectal cancer, a low anterior resection (LAR) removes the tumor while saving the anal sphincter if possible. Sometimes a temporary or permanent stoma (bag on the belly) is needed.
In the past, colorectal surgery required a long cut down the middle of the belly (20–30 cm). Recovery was painful – patients stayed in the hospital for 10–14 days. Today, with laparoscopic and robotic colectomy, Dr. Ravindra Vats makes only 4 to 6 tiny cuts (0.5–1 cm each). A small camera shows the entire colon and nearby lymph nodes on a big screen. Special long instruments remove the cancer safely.
Robotic colorectal surgery is even better for cancers in the rectum and low pelvis. The robotic arms have wrist-like movements that can reach deep into the pelvis. The 3D magnified view helps protect delicate nerves that control bladder and sexual function. Studies show that robotic rectal cancer surgery leads to better nerve preservation and lower rates of permanent stoma. Most patients leave the hospital in 4–7 days and return to normal activities within 3–4 weeks.
Surgeon makes 4–6 small cuts (0.5–1 cm) on the belly.
A high-definition camera shows the colon, tumor, and surrounding tissues.
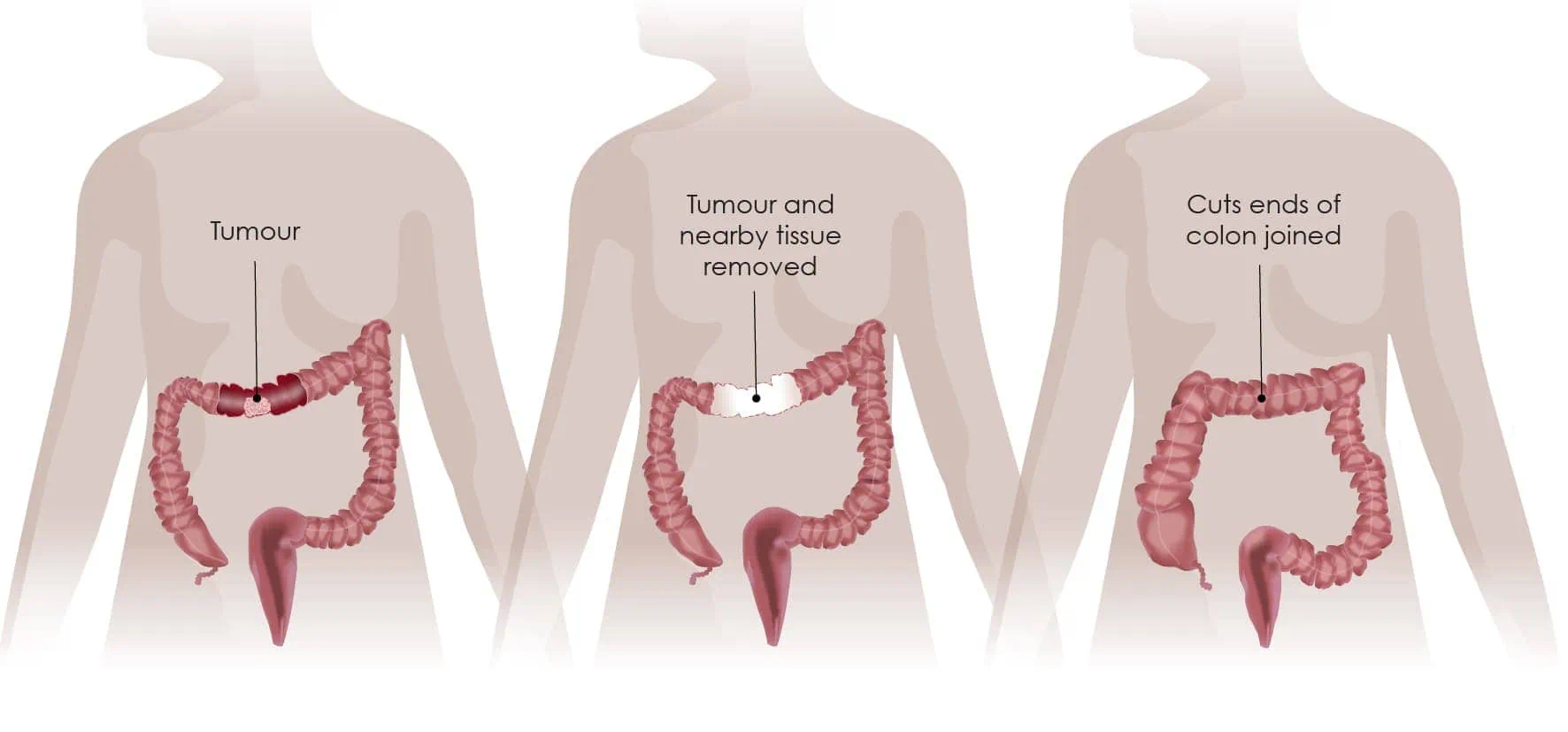
The cancer along with nearby lymph nodes is removed.
The healthy ends of the colon are stapled or sewn back together.
Tiny cuts mean much less pain. Patients need fewer or no strong painkillers.
Most patients go home in 4–7 days instead of 10–14 days with open surgery.
You can eat and pass stool sooner after surgery – usually by day 2 or 3.
Other benefits: less bleeding, lower risk of wound infection, fewer hernias at the incision site, and better cosmetic results. For rectal cancer, robotic surgery offers better nerve preservation – meaning lower risk of incontinence and sexual problems after surgery. Studies show that laparoscopic and robotic colorectal surgery have the same cancer cure rates as open surgery.
| Factor | Laparoscopic / Robotic | Open Surgery |
|---|---|---|
| Cut Size | 4–6 small cuts (0.5–1 cm) | One large cut (20–30 cm) |
| Hospital Stay | 4–7 days | 10–14 days | Pain Level | Mild to moderate | Severe |
| Return to Normal Diet | 3–4 weeks | 6–8 weeks |
| Procedure | Description | Recovery Time |
|---|---|---|
| Right Hemicolectomy | Removal of cecum, ascending colon, and part of transverse colon. | 4–6 weeks |
| Left Hemicolectomy / Sigmoid Colectomy | Removal of descending or sigmoid colon. | 4–6 weeks |
| Low Anterior Resection (LAR) | Removal of rectal cancer with preservation of anus. | 6–8 weeks |

We use 4K and 3D laparoscopes, robotic systems with fluorescence imaging, and advanced staplers for safe connections. Indocyanine green (ICG) dye helps us see blood supply to the colon during reconnection, which lowers the risk of leaks. For rectal cancer, we use transanal endoscopic surgery (TEMS/TAMIS) for very early tumors. All surgeries are done in ultra-clean operating rooms.
Book your consultation with Dr. Ravindra Vats and get trusted surgical care with advanced treatment.
Book Appointment